


The New Death Panels: Health Care Rationing Via Delays And Denials


There is a dark force that is rationing care to millions of Americans. It’s causing delays and denial of health care and increasing the cost of care for all of us. No, it’s not the deep state or The Pentaverate. This dark force is health insurance companies. The impact they are having is staggering and damaging.
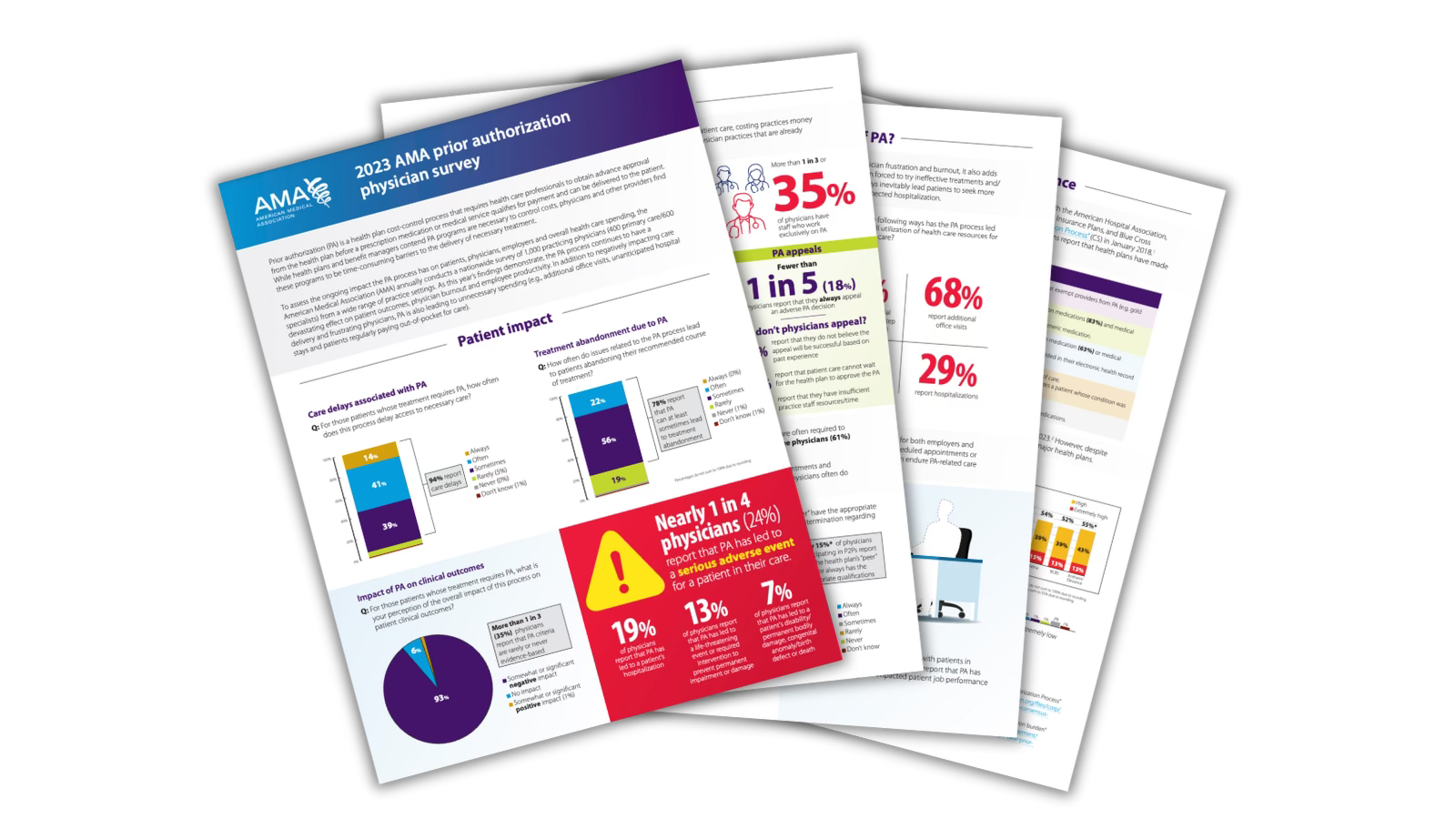
A recent American Medical Association survey of physicians produced some troubling results. More than 90% of responding physicians reported that prior authorizations required by insurance companies have a negative impact on patient clinical outcomes, and almost 80% reported that prior authorizations resulted in patients often or sometimes abandoning a recommended course of treatment.
Let that sink in for a moment. If you are as old as I am, you remember the uproar around the fear of “death panels,” when one-time vice-presidential candidate Sarah Palin said that under a provision of the Affordable Care Act proposed in 2009 by President Barack Obama, people “will have to stand in front of Obama’s ‘death panel’ so his bureaucrats can decide, based on a subjective judgement of their ‘level of productivity in society,’ whether they are worthy of health care.”
As we know, that didn’t happen. Unfortunately, a different form of these “panels” are already operating. Insurance companies are filling this role, and they are not basing their decisions on productivity but rather on profit.
Let’s look at some of the other data from the AMA survey.
One out of four doctors reported that prior authorization delays and denials led to a “serious adverse event” for their patients. Remember all the discussion about serious adverse events caused by the COVID vaccine? The data there point to an adverse-reaction rate far less than 1%.
And, amid a great deal of discussion lately about physician burnout, 95% of the doctors in this survey reported the prior-authorization process contributed to their feeling of burnout. My question here is, who are the doctors who don’t feel this way? Sort of like asking, if four out of five dentists recommend brushing your teeth, who is the fifth dentist?
Please read the whole survey; it is chilling.
Now, out of fairness, this is a survey and not a scientific analysis of payer denial data. The results are self-reported by the physicians who answered the survey. I would love to see a full analysis of payer denial and prior authorization, but to do that the payers would have to make all that data available. I have a better chance of winning a gold medal in the Olympics than we do of having the payers agree to that kind of transparency.
At this point I can hear the voices of the payers and their supporters: “We are doing this to protect patients from unproven or ineffective treatments.” Or, “There are bad doctors out there ordering things they shouldn’t.” Sure, there are bad doctors just like there are bad lawyers and bad plumbers. But should we believe that 90% of them are bad?
Here is the reality: Insurance companies are incentivized to deny care and to make it so hard to get care that the people who really need it will either give up or switch to a different insurance company. The big problem is, they are harming patients and burning out doctors in the name of profits and stock prices. If we don’t do something about this and demand better, this problem will only get worse.
The insurance companies are not going to change on their own. There is just too much money to be made by playing this game. It’s going to take legislation and most likely litigation to fix this. I am a free-market economist, so I tend not to like either of those solutions unless absolutely necessary. This is one of those cases when it’s necessary.
 | A guest post by
|
I agree with the general thesis of this post, and also that the AMA survey has to be taken with a large grain of salt because it was purely self-reporting and not data-based. However, no matter what healthcare reimbursement system is in place, it is a simple fact that costs must be controlled - funding is not, and never will be, infinite. The 3 major components of making expenditures reasonable will be: (1) Eliminate private insurance, and thereby cut out the current 20% or more of premium payments that go to exorbitant administrative overhead+executive salaries+ profit, rather than to patient care. In its place, implement a national single payer program - - which would NOT!! take over the *delivery* of healthcare, but would simply re-channel the collection & disbursement of healthcare dollars. With single-payer (think re-vamped Medicare covering all ages, and with improved/more equitable provider reimbursement), there would be no profit motive, executive salaries, or stockholders, and the overhead would amount to roughly only 5%. [For those who want to learn more about single-payer, check out Physicians for a National Health Program.] (2) Mandate drug price negotiation - just like Medicare is now beginning to do. (3) We must be clear-eyed and acknowledge that not all care recommended by a provider or desired by a patient is appropriate and necessary. And that more care is not always better care. I can attest to all of that as a physician who during my career saw a substantial amount of unnecessary or duplicative testing, procedures and referrals - mainly, I think, because providers are too pressed for time to do what we should be doing, which is to think and consider rather than the fastest and easiest route, which is to treat/order/refer. In addition, what we were trained to do in residency is not always (or does not always remain) best practice based on hard outcomes data. What will ultimately be needed are *physician*-devised and -managed, evidence-based, flexible guidelines. I had experience with these as a practitioner and executive at Kaiser Permanente for part of my career, and they can be successfully implemented and effective.
AI has accelerated this problem. People setting the rules for AI are not using data to support their denials. They simply "think" that this shouldn't be covered versus using scientific data supporting the denial.